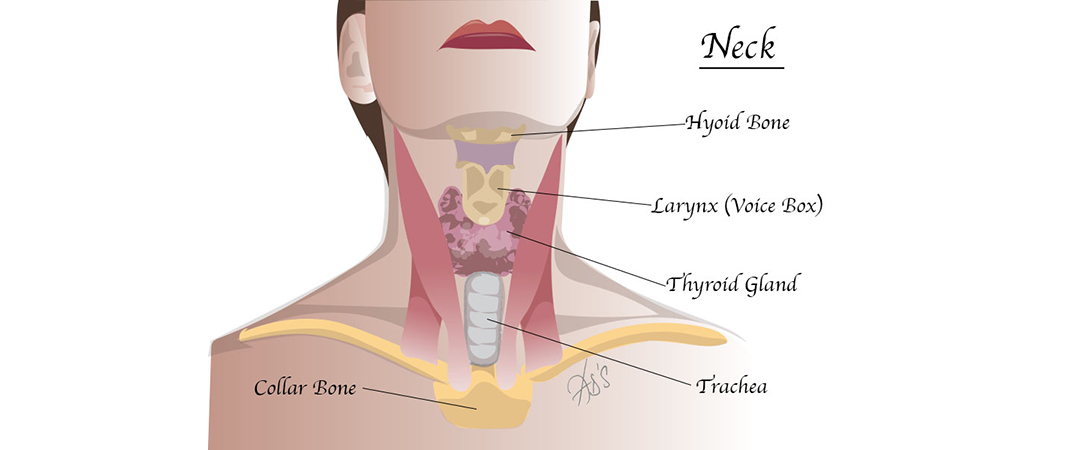
The thyroid gland lies in front of the neck just below the Adam’s apple. It is butterfly shaped. The right and left wings (lobes) are joined by a small bridge of thyroid tissue (body) called the isthmus, and surround the windpipe. The thyroid gland manufactures thyroid hormones, which are chemicals that are essential for survival.
Any enlargement of the thyroid gland is called goitre. When the whole gland is enlarged it is called a diffuse goitre. If there is a single nodule, it is termed a solitary nodule. The majority of goitres are not cancerous, but a small proportion of goitres may harbour cancer cells. Therefore all thyroid swellings should be investigated by an ENT specialist.
During the consultation, a detailed history the problem is noted and an examination is carried out. This is followed by an ultrasound scan, during which a needle may be inserted into the lump to collect a sample of cells, this is called fine needle aspiration cytology test (FNAC). These cells are analysed under the microscope to determine the nature of the growth.
Other tests, such as a CT scan, MRI scan or nuclear isotope scan which may be required in some cases. Often no treatment may be necessary and you will be advised to adopt a ‘watch and wait policy’.
Alternatively, surgery may be advised. This is commonly undertaken when there is a suspicion of cancer, pressure symptoms (problem swallowing or tightness in the neck and chest etc.), altered activity, and cosmetic concerns. The surgery is called Thyroidectomy and is explained briefly below.
There are different terms used to describe thyroid surgery. The following is a summary:
The risks involved are significant but are rare and will be discussed before surgery:
If the entire thyroid gland is removed you will need to take replacement thyroid hormone, thyroxine (T4) in tablet form indefinitely. The amount of thyroxine needed will be monitored based on blood tests.
If only part of the thyroid gland is removed, then no hormone replacement is required and the remaining gland will produce enough hormones to meet the demands of the body. Blood tests will be done to confirm this after the operation.

PRACTICE MANAGER: Chelsea Fulton 07534 771264 MEDICAL SECRETARY: Karen Harris 07453 881588
CORRESPONDENCE ADDRESS: Enso House Crayfields Business Park, 3 New Mill Road, Orpington BR5 3TW